Title:
"Twist of Fate?"
Complexity Level:
🟠

A 32-year-old woman with a history of diabetes mellitus presents to the Emergency Department with blood glucose levels exceeding 400 mg/dL. She also reports experiencing atypical chest pain.
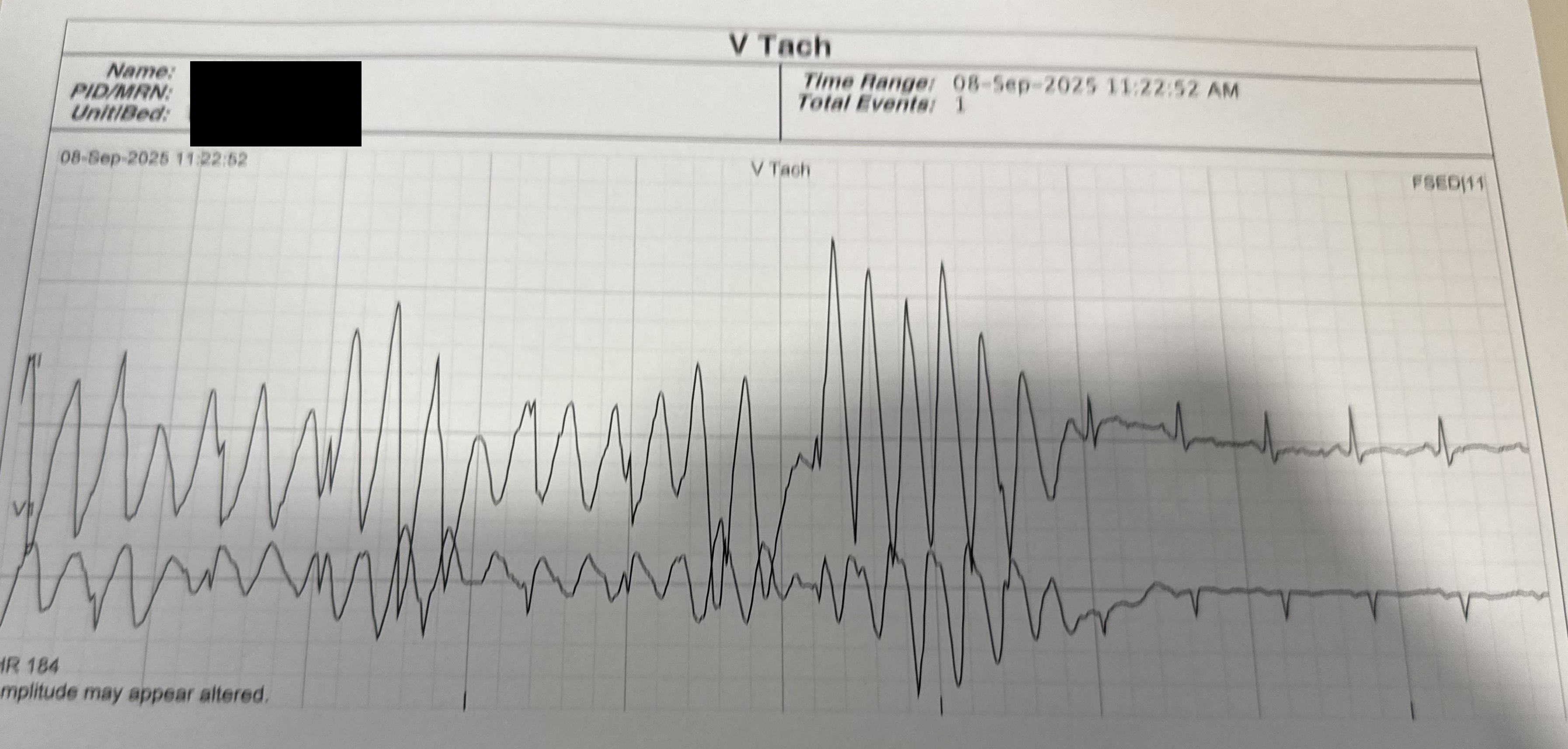
While being monitored in the ED, her telemetry shows intermittent episodes of wide QRS complexes at a rapid rate.
What's the most appropriate next step?
[reveal correct="d"] Your explanation content here... [/reveal]

Correct answer is A. Explanation in video below.
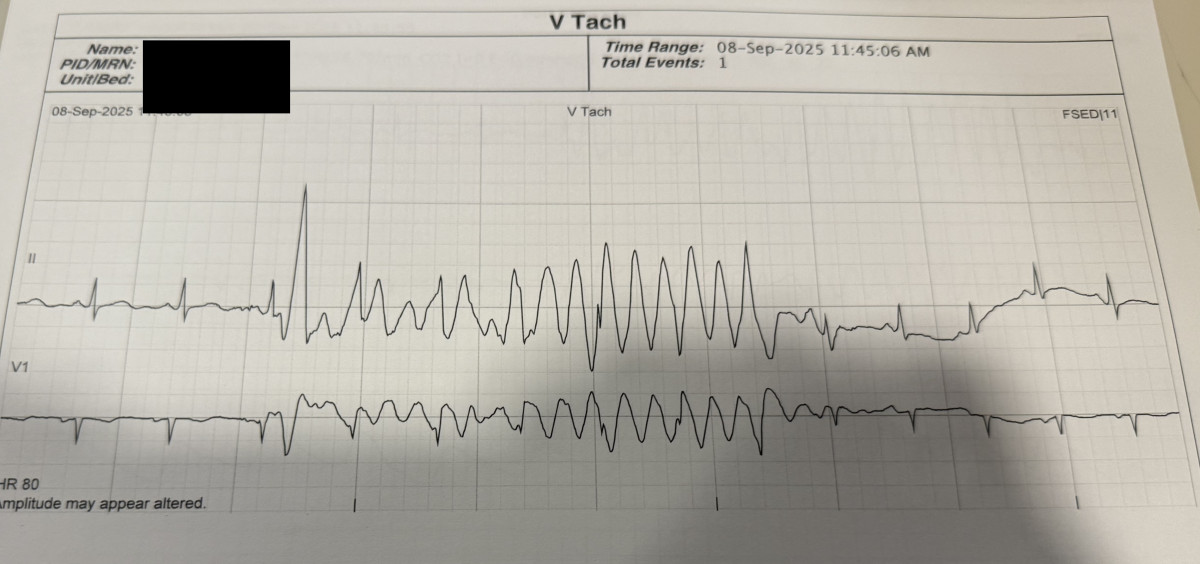
Since most people (over 60%) voted to treat this as torsade, it’s worth clarifying why this is actually artifact rather than a true arrhythmia. The strip mimics polymorphic VT, but several key features are missing:
✅ Teaching point:
Because artifact can mimic polymorphic VT, many clinicians may mistake it for torsade. Recognizing the absence of QT prolongation and the lack of pause-dependent initiation at the red arrow is key.
📌 One-liner takeaway:
If there’s no pause and no QT prolongation at initiation (red arrow), it’s likely not torsade.