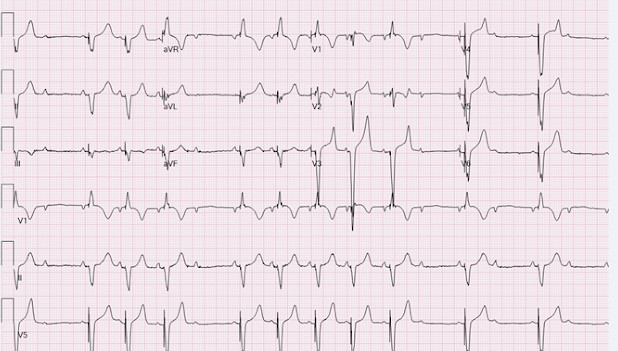
A 73 year old male patient with history of cardiomyopathy and complete heart block s/p biV ICD. He was recently seen by a cardiologist and had a programming change made since he has been complaining of dyspnea on exertion and some dizziness. EKG is shown.


Thanks for the case @Yousef Darrat.
There is a clear intermittent non-tracking of P waves, with no ventricular spikes fired, hence pauses that are likely causing his dizziness.
"Ventricular non-capture" is incorrect since there is no visible ventricular spikes fired with no QRS following them. "RV under-sensing" will cause the opposite (i.e., inappropriate ventricular spikes fired), which we don't see here.
"RV oversensing", which is in general very rare, may explain the absence of ventricular spikes, however, this is unlikely, unless it is very random and intermittent. Also, this has to be proven using EGM for PM to that will explain the mechanism of oversenting. Moreover, the absence of ventricular firing here is appears to be somewhat systematic with only certain P wave not followed by ventricular tracking, which will make it more suspicious for a functional behavior of the device, leading to ignoring some of the "P" waves (overlooked).
Although his sinus rate is at or slightly above 100 bpm, will vote for "upper rate behavior", although that is usually seen at very high-tracking rates close to the 130 bpm by default in most devices. I suspect that it is likely induced by the programming change made by his cardiologist, especially if that involves factors affecting total atrial refractory period (TARP, i.e., PVARP and AVI).
Thanks Fathi for your comments, Agree upper rate behavior, as you mentioned if P waves falls in TARP (AV delay+PVARP) then it will not be tracked and patient will have 2:1 block as in this case.
Thanks @Yousef Darrat .
QRS in best #8 looks distinctly different than rest of beats (best seen in V1/V2). Any thoughts about that?
@Fathi Idris
Since the patient has complete AV block and dependent most likely it is a PVC fused with paced complex, other possibility anodal capture although I do not think device is programmed to RV tip. What are your thoughts?
Agree. In CRT whenever morphology changes you will consider loss of capture in one lead, especially left, but this happens in one beat and is still relatively narrow, so likely a fortuitous PVC fuses with paced beats.