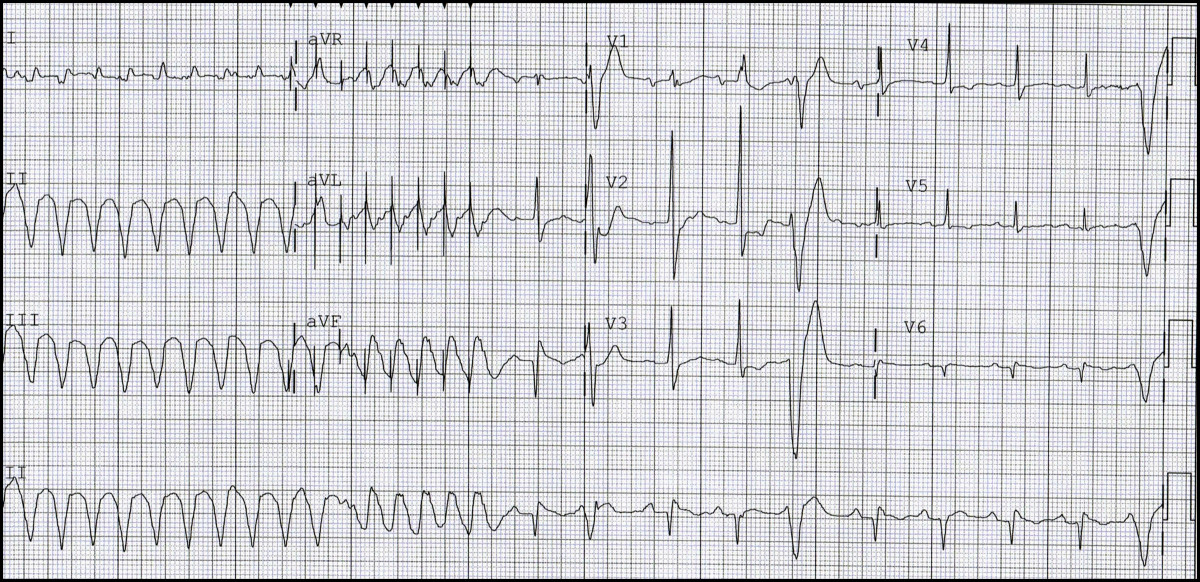
A run of ventricular tachycardia (VT) followed by anti-tachycardia pacing (ATP) leading to termination of the arrhythmia.
Discussion
The most interesting part of the tracing is the initial run of wide QRS tachycardia. This is suspicious of VT. A close look at the morphology of this run shows that the initial ten beats look different than the last six beats. Leads AVR and AVL clearly display pacing spikes preceding the last eight beats of the run. The wide QRS tachycardia seems to terminate after these paced beats. This is not a matter of chance, so how did it happen?
The patient likely has an implantable cardioverter defibrillator (ICD) and the initial part of the tracing shows a run of VT. This arrhythmia was recognized by the ICD, which was then triggered to pace in the right ventricle at a rate faster than the VT, hence overdrives the ventricle and colloids with and terminates this VT. This feature is called “anti-tachycardia pacing” or ATP.
When more history was obtained, the patient indicated that he has previous heart attacks and a “weak” heart muscle. He has an ICD implanted several years ago. Device interrogation indicated that he has had more than 600 episodes of VT in the two days before presentation; all of them were treated successfully by this ATP function. Catching ATP on a 12 lead EKG is not a common encounter, and this may reflect the very frequent episodes that this patient had.
Fig. 2 and Fig. 3 were taken from the ICD interrogation with illustrations added to explain the presenting EKG. In these figures, the top two channels represent atrial and ventricular activities respectively; the middle channel is a channel marker, while the bottom one shows the cycle lengths. (AS) indicates sensed atrial activities, and (VS) indicates sensed ventricular activities. In this kind of device, fast ventricular activities are labeled “T2”.
In Fig. 2, the initial part of the tracing represents normal sinus rhythm with atrial activities preceding ventricular activities, this sequence is illustrated by the blue tilted arrows. After six sinus beats, the ventricular rate, suddenly, increased (blue dots) while atrial activities at the top channel remained unchanged. This is a run of VT with AV dissociation. The device recognized this and labeled it “T2” (end of tracing in Fig. 2).
Figure 2 - Intracardiac electrograms- Sinus rhythm (arrows) followed by VT (dots).
In Fig. 3, the first eight beats (blue dots) represent a continuation of the VT, as shown in Fig. 2; this was followed by a six-beat run of a different morphology (blue stars), which is a bit faster. These are paced beats -labeled “STIM” by the device (also, marked as ATP)- which led to termination of tachycardia and establishment of normal sinus rhythm.
Figure 3 - Intracardiac electrograms - VT (dots) followed by ATP (stars) leading to sinus rhythm.
Although available in most recent devices, ATP is generally underappreciated by non-specialized practitioners, who tend to think of ICDs as “shocking” devices only. In fact, this function can be extremely helpful in treating patients with ventricular tachycardia that meet certain criteria, leading to a “painless”, i.e., without a shock, termination of the arrhythmia. The details of this function are beyond the scope of this short vignette.
The patient was treated with Sotalol, and was doing well at a 3-month follow up.

F
Answer:
A run of ventricular tachycardia (VT) followed by anti-tachycardia pacing (ATP) leading to termination of the arrhythmia.
Discussion
The most interesting part of the tracing is the initial run of wide QRS tachycardia. This is suspicious of VT. A close look at the morphology of this run shows that the initial ten beats look different than the last six beats. Leads AVR and AVL clearly display pacing spikes preceding the last eight beats of the run. The wide QRS tachycardia seems to terminate after these paced beats. This is not a matter of chance, so how did it happen?
The patient likely has an implantable cardioverter defibrillator (ICD) and the initial part of the tracing shows a run of VT. This arrhythmia was recognized by the ICD, which was then triggered to pace in the right ventricle at a rate faster than the VT, hence overdrives the ventricle and colloids with and terminates this VT. This feature is called “anti-tachycardia pacing” or ATP.
When more history was obtained, the patient indicated that he has previous heart attacks and a “weak” heart muscle. He has an ICD implanted several years ago. Device interrogation indicated that he has had more than 600 episodes of VT in the two days before presentation; all of them were treated successfully by this ATP function. Catching ATP on a 12 lead EKG is not a common encounter, and this may reflect the very frequent episodes that this patient had.
Fig. 2 and Fig. 3 were taken from the ICD interrogation with illustrations added to explain the presenting EKG. In these figures, the top two channels represent atrial and ventricular activities respectively; the middle channel is a channel marker, while the bottom one shows the cycle lengths. (AS) indicates sensed atrial activities, and (VS) indicates sensed ventricular activities. In this kind of device, fast ventricular activities are labeled “T2”.
In Fig. 2, the initial part of the tracing represents normal sinus rhythm with atrial activities preceding ventricular activities, this sequence is illustrated by the blue tilted arrows. After six sinus beats, the ventricular rate, suddenly, increased (blue dots) while atrial activities at the top channel remained unchanged. This is a run of VT with AV dissociation. The device recognized this and labeled it “T2” (end of tracing in Fig. 2).
Figure 2 - Intracardiac electrograms- Sinus rhythm (arrows) followed by VT (dots).
In Fig. 3, the first eight beats (blue dots) represent a continuation of the VT, as shown in Fig. 2; this was followed by a six-beat run of a different morphology (blue stars), which is a bit faster. These are paced beats -labeled “STIM” by the device (also, marked as ATP)- which led to termination of tachycardia and establishment of normal sinus rhythm.
Although available in most recent devices, ATP is generally underappreciated by non-specialized practitioners, who tend to think of ICDs as “shocking” devices only. In fact, this function can be extremely helpful in treating patients with ventricular tachycardia that meet certain criteria, leading to a “painless”, i.e., without a shock, termination of the arrhythmia. The details of this function are beyond the scope of this short vignette.
The patient was treated with Sotalol, and was doing well at a 3-month follow up.