Note: This case have several images to be unfolded during discussion/interactions
A 68-year-old man presented with fatigue and shortness of breath for several weeks.
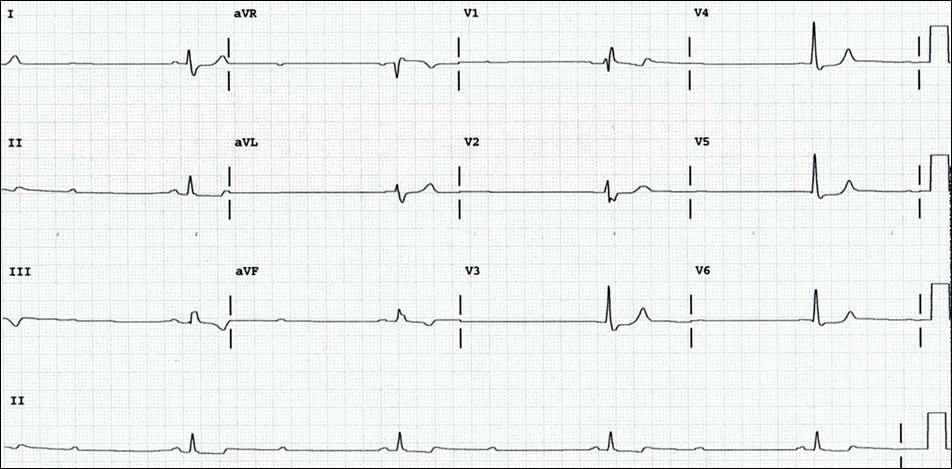
On an exam, he was found to have a slow heart rate. His EKG is shown below.
1-What is the interpretation?
2-What is the next step?

F
This tracing confirms that atrial lead is not capturing the atrium, but it appear to be firing at a rate less than 75 bpm, which means it senses "something" that resets the PM.
So, the atrial lead is likely dislodged and when this tracing was taking is just passed the TV and hence was partially sensing the ventricle (to reset the timer) but does not capture the ventricle.
Illustration below...
On the top of the EKG tracing the machine will mark the location of the PM spikes (black short vertical lines at the top of the EKG). At the early part of the tracing, you can see that the PM fires regularly at 75 bpm (except for the first spike), however, after that it will fire at a slower rate (the distance between PM spikes gets wider than the programmed rate). This indicates that the PM was sensing something and hence adjusts its pacing cycle accordingly.
The spikes seem to be occurring at a consistent distance from the preceding QRS complex (black arrows) which is the same timing cycle of the PM (red arrows - about 800 milliseconds). This suggests that the PM is probably using the QRS complexes to set its timing cycle (in most part), and hence it is probably sensing these QRS complexes (likely intermittently due to lead instability, which explains the lack of consistency – note it failed to sense some of the QRS complexes like the second beat on the tracing (*)), so it should be close to the RV (i.e., the TV area, likely just passed the TV).
The EKG below was taken while the PM was programmed in AAI mode LR of 60 bpm with the patient doing some maneuvers to assess lead stability. What is happening now?
Curious, was the maneuver to hold his breath in expiration.
Also, I did notice that after the native beat, the pacer sensing the ventricular activity. Also the pacing rate was around 70 bpm (the last two beats), I don't know why
excellent educational case!
Not clear for me , can we discuss the case by interactive video discussion?
F
Sorry, Naser. I just saw this. Will be happy to clarify further in a meeting.
Since device is programmed to AAI, all paced beats here are captured by atrial lead. The first 7 beats are ventricular paced beats (red circle) has superior axis, hence the lead is probably deep in low RV or even apical.
After that the PM then fails to capture the ventricle with subsequent emergence of the native sinus beat (beat # 8).
This is followed by three more ventricular paced beats (blue circle). Note that the morphology of these last three paced beats in the rhythm very bottom rhythm strip lead II is different (positive QRS, i.e., inferior axis) than the morphology of the first 7 paced beats (negative QRS, i.e., superior axis). This suggests that RV in these last 3 beats is captured in high RV (?RVOT or high-septal area with inferior axis).
The loss of capture in the middle of EKG and then change of morphology in the last few beats support that the atrial lead was floating around in the RV giving all the above confusing/inconsistent findings.
Now, if we go back and look at the EKG in Fig.2a again. Since the PM was in DDD mode, the first spike should be an atrial spike and the second ventricular.
When two spikes are there, the failure of atrial capture is easy to figure out, but since the first spike has to be an atrial spike, then beats #1, 4, 7 and 10 should be produced by the atrial lead now passing through the TV and capturing the neighboring septal area of RV (hence the QRS is narrow like Mansour pointed out, and with inferior axis).
It is hard to explain why the RV is captured a trigemini pattern, which can be fortuitous, or probably related the lead movement is being somehow affected by the patient’s respiration or position.
Finally, below is the PM programmer while testing this PM when programmed to AAI and DDD respectively:
The lead was revised and repositioned successfully.
Conclusion:
In general lead malfunction is easy to diagnose and figure out when it gives consistent finding on EKG.
Nonetheless, intermittent malfunction, or dislodged leads that migrates between different chambers, or “floating”, like in this case can create quite confusing EKGs with challenging interpretation.
Applying basic pacing timing interval principles and programming troubleshooting with or without maneuvers and, of course, CXR evaluation help sort this out.
Thank you for sharing this case with us.
بارك الله فيك ورحم الله والديك يا د فتحي وفي كل المشاركين