
Inferior STEMI can be because of lesions in either the right coronary artery (RCA) (most common), or left circumflex artery (LCX). The standard of care is to treat STEMI with urgent cardiac catheterization and PCI.
However, evaluating the EKG before taking the patient to Cath lab may give the operator a hint about the potential culprit vessel and hence may help to plan the procedure.
This quiz is based on two actual cases of inferior STEMI to discuss this concept.
- Case 1: A 55-year-old male who presented with h/o DM, smoking and hyperlipemia in ER with SOB and diaphoresis.
- Case 2: A 67-year-old-male with h/o CAD and prior stents. He presented with successfully resuscitated cardiac arrest after a brief episode of CP.
- Where is the lesion for these two case?
- 1-Case 1: RCA & Case 2: LCX
- 2-Case 1: LCX & Case 2: RCA
- 3-Both cases: RCA
- 4-Both cases: LCX
- 5-Not enough information to be conclusive


Comments
F
Correct Answer is: 1 (Case 1: RCA & Case 2: LCX)
In Case of inferior STEMI, it is useful to use the algorithm proposed by Zimetbaum et al. for localizing the lesion (N Engl J Med 2003 Mar 6;348(10):933-40. doi: 10.1056/NEJMra022700.). (see diagram below)
You start simply by looking for two findings: III/II ratio and reciprocal ST-changes in I & aVL.
Case 1:
By looking at III/II ratio and ST-changes in I & aVL, first It looks like that ST elevation in III>II. Second, there are notable reciprocal changes in I & aVL (ST depression). This combination will have 90% sensitive and 94% PPV for RCA lesions (see diagram below).
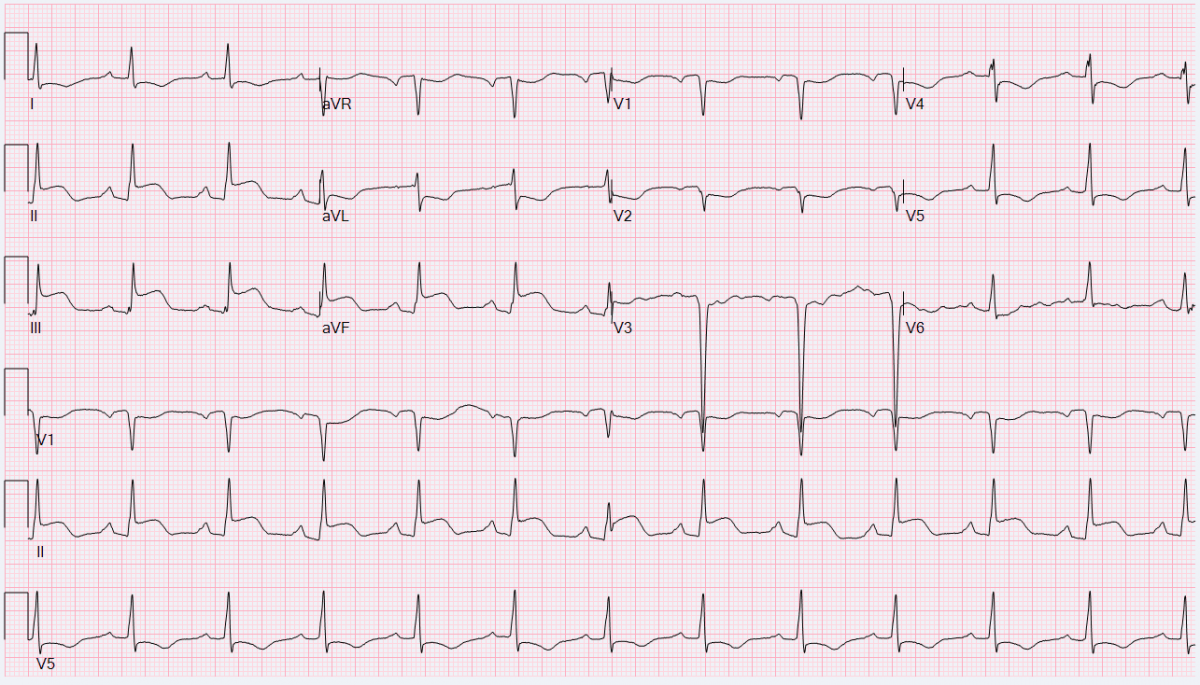
Case 2:
Again by looking at III/II ratio and ST-changes in I & aVL, it looks that ST elevations in III and II are comparable, and there are no impressive reciprocal changes in I & aVL. This will make it suspicious for LCX lesion.
We then look at chest lead for more confirmatory findings: ST depression in antero-septal leads V1-V3 (equivalent to ST elevation in posterior leads!) and ST elevation in lateral leads (I, aVL, V5, and V6).
Here we can see that there is ST-depression in V1-V3, and ST-elevation in V5, V6. Based on the algorithm, these findings are 96% specific for LCX lesion with a PPV over 91%.
Tip / Take-home message:
In RCA lesions remember 2 Rs: Ratio of (III>II) ST elevation, and Reciprocal changes (depression) in I & aVL. If present, then it is likely RCA lesion.
If not, then look for more ST elevation to confirm your suspicion about LCX (V1-V3 st depression which is posterior elevation, V5-V6, I, aVL are lateral elevations which are usually LCX territories).
Inferior STEMI localization Algorithm: