
I need your help and guidance about this current patient I have.
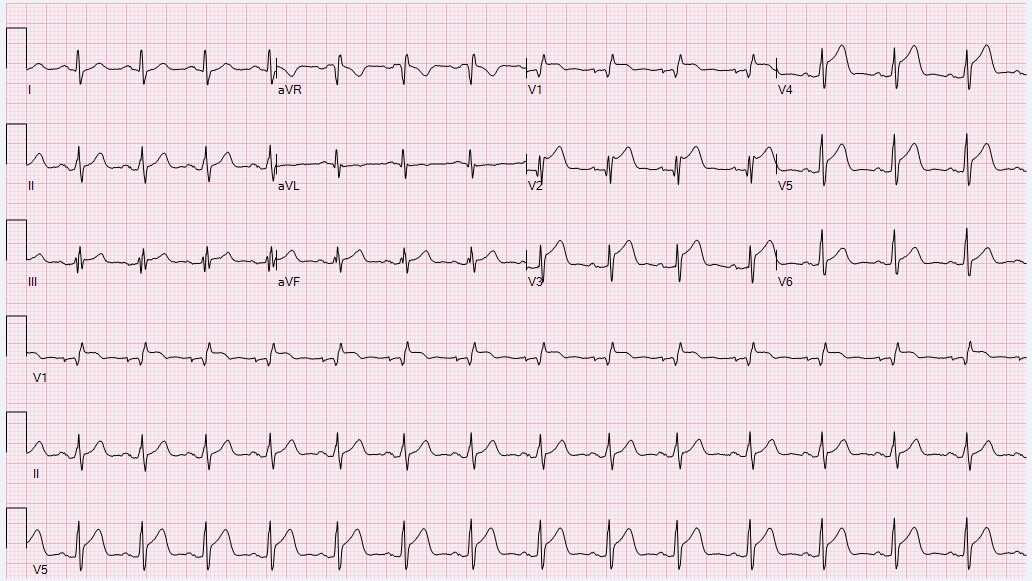
This is a 55-year-old male with history of diabetes and hyperlipidemia. He presented to another hospital in June with anterior wall STEMI (EKG shown).
He underwent PCI to LAD, unfortunately was a tough case with suboptimal result. He also has severe disease as shown in the attached angios.
He then switch care to us and we are following him for the last 2 months. He is completely asymptomatic and very functional and does active labor work with no restrictions. His echocardiogram showed an ejection fraction of 35-40% roughly.
his cardiac MRI shows nonviable anterior wall in the middle and apical segments. There was also some inferolateral infarct. There was a comment about mild inferior hypokinesis. Ejection fraction by MRI is 39%.
His currently on reasonable medical therapy including dual antiplatelet therapy, statin, carvedilol, Ace inhibitors. Just switched to Entresto a couple of days ago. His blood pressure soft and pushing medicine further may be a challenge.
Questions:
-Would he benefit from PCI to RCA ( can he fit COMPLETE trial picture)?
-How about ICD?
F
COMPLETE Trial:
https://www.acc.org/latest-in-cardiology/clinical-trials/2019/08/30/21/28/complete
F
Tnx. @Khaled Sleik . Anterior wall is non-viable. Also, infero-lateral scarring (not sure how big). RCA is easy to fix, but Cx is a CTO.
Circumflex is very small and gain is little and CTO ( infero lateral scarring ?)
RCA looks easy but I think will very difficult ( depends in few factors) guide support and degree of calcium beside there is mid segment lesion in addition
F
@Khalid Abozguia @Yousef Darrat would you give this man an ICD now?
F
Thanks @Khalid Abozguia . His EF is 39% (just below 40%), which based on current guidelines make him qualified for ICD (MADIT-II), NYHA-II.
Is the reason you don't vote for ICD yet because he has been on GDMT for only 2-3 months?
His is already on Farxiga (added by his PCP). Regardless, MADIT-II was conducted before SGLTI showed mortality benefit. So, it will be interesting to show that SGLTI blunt the benefit added by ICD placement, just curious).
If so, who long would you wait before you re-check his EF and decide about ICD?
MADIT II LVEF < 30%
guideline now recommend ICD :
< 35% if NYHA II-III
or
< 30 % even if NYHA I
or
< 40% + NSVT - MUSTT study recommend VT stim (EP study) - if positive then ICD
F
Sorry Khalid, I meant 35% (not 40%, but >40 days post MI) and NYHA-II. His EF by MRI is just above that (39%) which with degree of scarring he has makes me wonder if it will not get any better. Last year I had a patient argued with me on his EF of 38% why not implant ICD. It turned out that he will get disability if he gets ICD, but since I didn't implant it, he fired me!
F
Conclusion:
At last visit, we discuss all options with the patient. The plan was to push GDMT to the highest tolerated dose for next 3 mo and then re-evaluate him. Life-vest was discussed with him but of course was not approved since his EF is still above 35%.
Will keep you updated on his future progression. tnx you all for help in this case.