A 41-year-old lady who presented with syncope. In the emergency room, her high sensitivity troponin went from 48 to 183 in 1 hour. She reported mild shortness of breath and chest pain on exertion.
What was the likely mechanism of her syncope? (answered in the 1st comment)

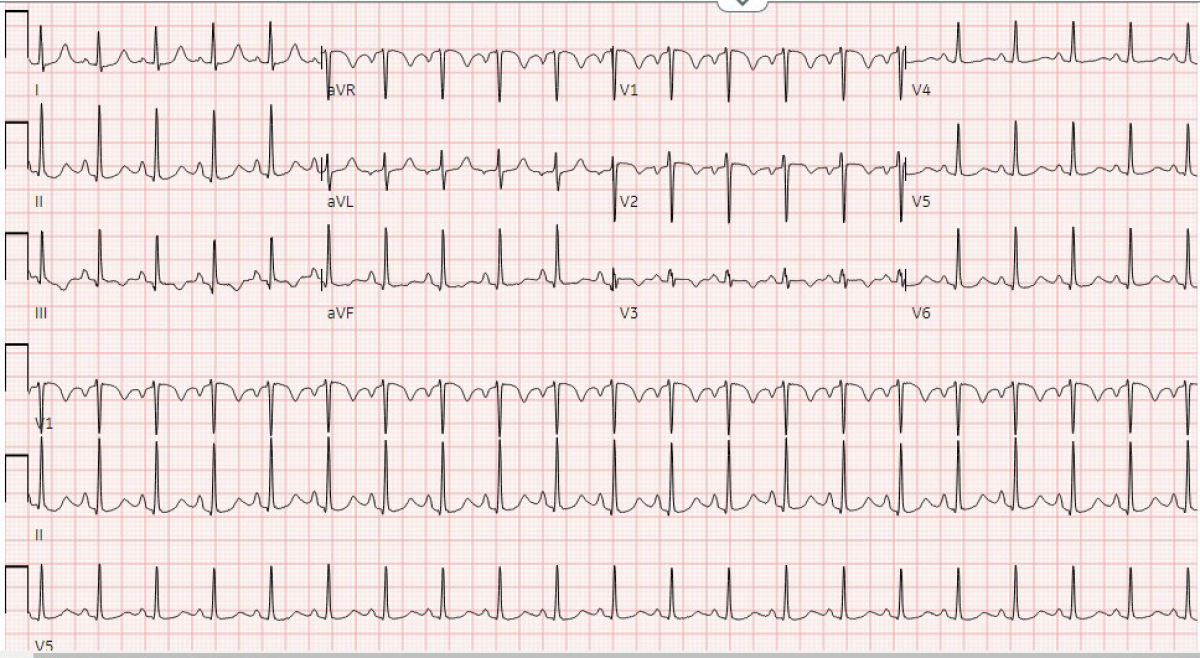

The EKG shows sinus tachycardia. In addition, there are few other subtle abnormalities that are relevant in this case. The P-wave is slightly told suggestive of possible right atrial abnormality. In addition, there is clear T-wave inversion in leads V1 through V3. This T-wave changes, in addition to the slightly elevated troponin may raise suspicion about ischemia, however, the clinical scenario of syncope, and shortness of breath, should all was raise suspicion about massive pulmonary embolism causing similar changes as well (the slightly elevated troponin, and T-wave inversion, may in fact represent right ventricular ischemia/injury due to strain from massive PE, leading to syncope).
Moreover, her EKG shows other suspicious changes (a small R-wave in lead 1, and a Q-wave, as well as inverted T-wave in lead 3). Put together, these findings are very suspicious for massive pulmonary embolus leading to syncope by a transient interruption of pulmonary circulation.
Apparently, the patient was released from the hospital a few days earlier after prolonged stay for thigh abscess surgery. Her CT scan confirmed the presence of massive pulmonary embolus. Her echocardiogram showed classical signs of RV strain.