
I want to share this "routine" case we see everyday, but it has a little twist that we don't see very often. No tricks here!!
This is a 41-y-o Hispanic male, presented with lingering CP x 12 hrs. Exam negative.
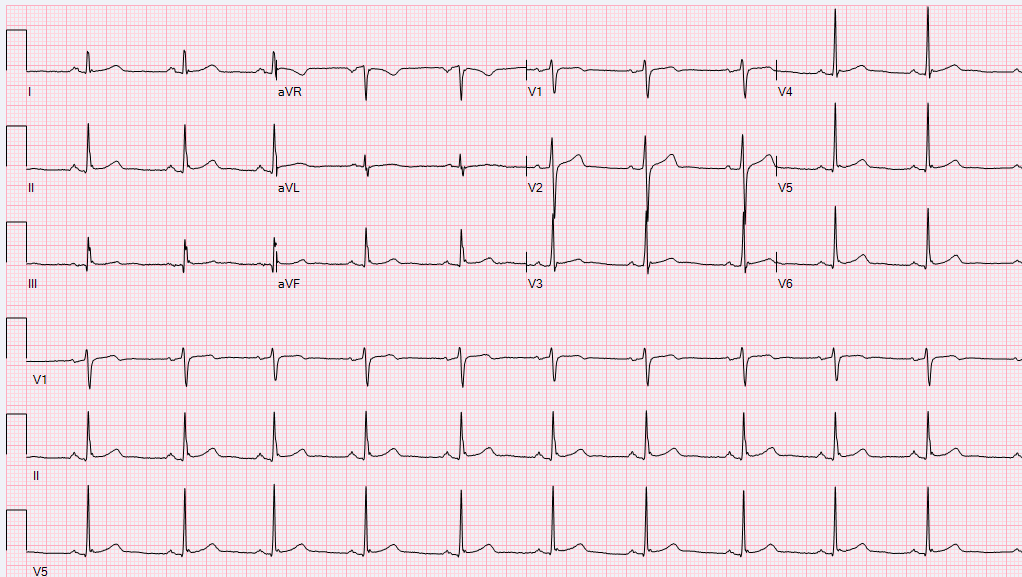
Presenting EKG below:
Troponins below:
Did well overnight. No recurrent CP.
What's next: Stress or Cath?
Comments
F
Well, here is the rest of the case. The resident order a stress test, plain treadmill test. The tracings are shown below.
F
At the end of the stress test, the patient was completely pain-free with no symptoms. Nonetheless, cardiac catheterization was performed promptly given the remarkable EKG changes on the treadmill.
This essentially showed 2 lesions, 1 in the LAD distribution and the other 1 in the RCA distributions. Images are below.
F
The LAD lesion was expected based on the stress test finding, and the Wellens pattern, however the RCA was unexpected. However, compared to the LAD lesion, the RCA lesion looked more hazy and suspicious for being an active plaque. The temptation was to do one lesion at this time, and leave the other one to be staged after assuring the patient's compliance with dual antiplatelet therapy.
Unfortunately, OCT equipment was down, therefore intra coronary imaging was not performed to delineate the exact nature of this lesion. Therefore, both lesions in the being stented. However, I am not completely sure, that was the most appropriate decision.
Caveats: