

a 49-year-old female with PMH of hypertension, Type II diabetes, and dyslipidemia
She comes to our clinic with 3 months history of atypical chest pain and DOE. She describes her pain as diffuse precordial aching pain, which happens randomly and is not related to exercise. It lasts for a few minutes, and nothing alleviates her pain. She also has worsening DOE over the past 3 months, ROS is otherwise negative.
Physical exam: is not remarkable
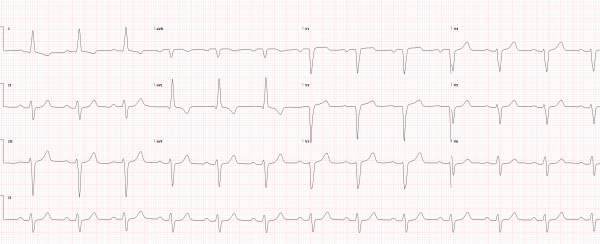
EKG as below
Labs work CBC, renal function and liver function are within normal limits, LDL 73, HDL 75, TG 162, cholesterol 193, HgA1c: 12%. No troponin was ordered.
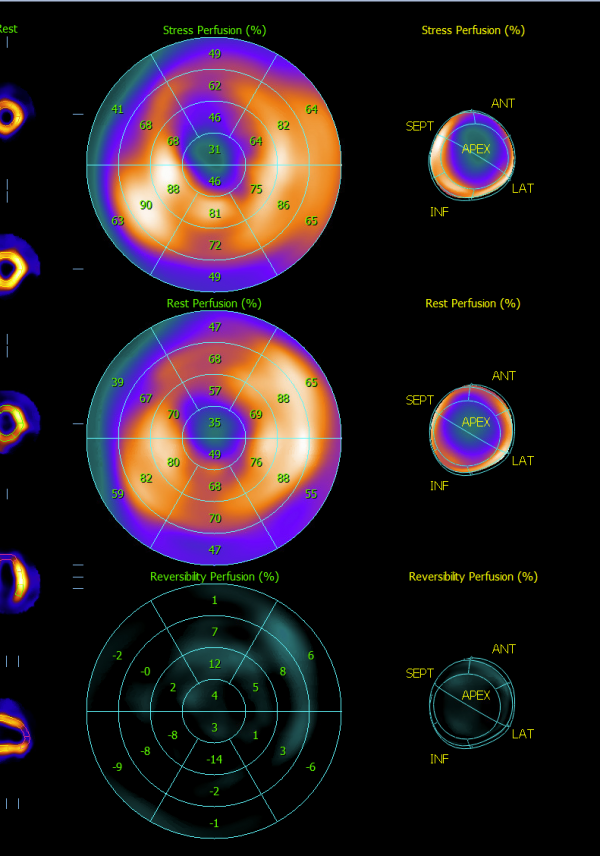
A myocardial perfusion study ( LExiscan) showed: a large fixed apical defect, and moderate anterior wall ischemia, see image below
Transthoracic Echo: EF 45-49%, apical akinesis, grade II LV diastolic dysfunction, LAV index 45 ml/m2
We proceeded with Coronary angiography ( see video below)
What is the diagnosis? what is the best next test? and how would you treat it?
https://drive.google.com/file/d/1_Ep_NDU0-O8h3o1C1cIsE_T0p4XE0Jck/view?usp=share_link
try the link to view the video
Thank you
@Saif El Nawaa . It is better to use either (Full post or Discussion) to post such a detailed case. You can have more control on uploads. Video is re-uploaded here.
I did not know about the full post, I will make sure I will do it next time insha allah thank you
I do not think her symptoms of chest pain are related but certainly her dyspnea could be.
12-lead EKG showed sinus rhythm, left atrial enlargement and left anterior fascicular block (LAFB).
Coronary angiogram showed right dominant circulation . Coronary arteries ectasia with right to left collaterals. Coronary CTA might be helpful.
will wait for more answers and I will post the CT for you
A
You can see the contrast washing at the LM, and looks connected to another vessel, most likely pulmonary artery. ALCAPA (anomalous origin of left coronary artery from pulmonary artery). Usually detected earlier in life. Symptoms can vary from CP to SOB and can cause a CMP. Over the years R-L collaterals develop and help with symptoms. Main way to treat this condition is surgically. Either ligation of LM and bypassing with a LIMA or reimplantation of the LM it the left coronary cusp and creating a neo ostia. Not common, I was lucky enough to see one so far and she was in her early forties. Nice case :)
Excellent summary for the diagnosis and the treatment
we will refer her to Houston for her surgery ( likely left main reimplantation)
F
Agree with @Ali Elfandi. Aberrant origin of LM from a lower pressure circulation (likely pulmonary system). Suspect a good size L-to-R shunt with potential heamodynamic effect.
Never seen case before. @Saif El Nawaa I think you should right it up!
Thank you Ali for your input!!!
This is the CT