
Dear colleagues/friends,
I need your help with a case that we saw last week. I am not sure we know exactly what is going on with her. I am wondering if you see a similar case before, or how would you manage her if she is yours. Will tell you later what we decided to do.
Appreciate your help!
tnx
History:
66-year-old female with PMH significant for hypertension, type 2 diabetes mellitus, and chronic pain (followed at pain clinic) presents to ED for evaluation of chest pain.
Patient reports intermittent sharp, achy chest pain beginning 3 days ago. Mostly located above and around left breast with some radiation into left arm. She also reports mid upper back pain at times. Exacerbated with deep breaths but denies alleviating factors.
She denies prior hx of DVT/PE, recent prolonged travel, recent surgeries. Denies fever, chills, palpitations.
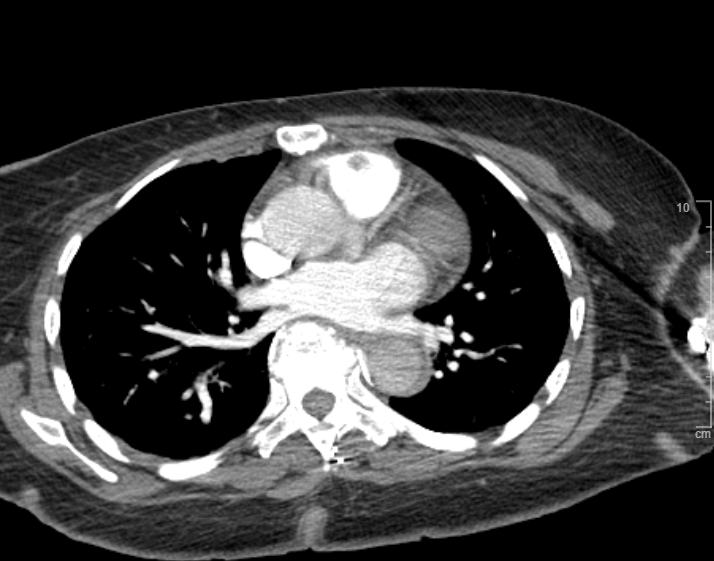
ED workup mostly unremarkable but D-Dimer is elevated at 1580. Chest x-ray negative for acute process. CT a chest showed filling defect pulmonic valve. Questionable for focal thrombus, potentially infected vegetation, or soft tissue mass/neoplasm.
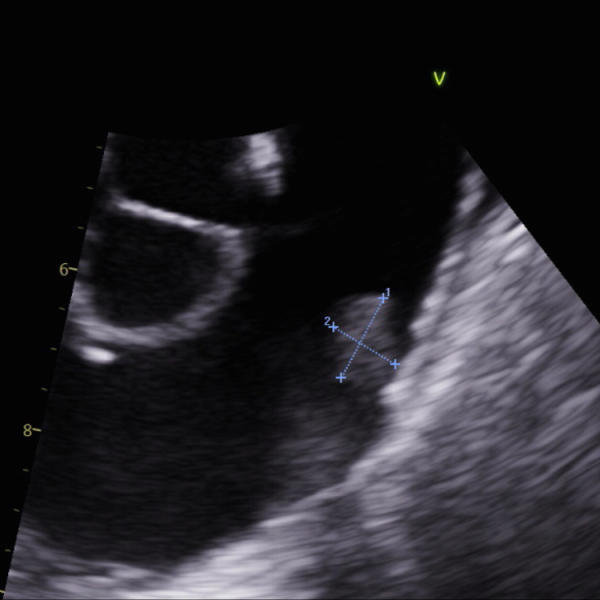
Attached images from CT (with contrast) and TEE.


This is most likely pulmonary artery sarcoma required surgical removal it will increase in size and cause obstructive symptoms . Rare tumor likely unrelated to patient symptoms.
F
Thanks Khaled. Suspicious for tumor. Two questions:
Thank you Dr Fathi for sharing this interesting case. I reviewed this case report on pulmonary artery sarcomas. about 50 percent of these tumors apparently are initially misdiagnosed as PE. Options for diagnosis include MRI (higher T2 intensity compared to embolisms), FDG (PET scan ) can show increased uptake. In this case report the diagnosis was established via Endobronchial ultrasound (EBUS) and FNA. I would love to hear how you proceeded with this case.
No idea why Ddimer elevated possible cancer!!
no obstructive features you could wait and watch for now without surgery
get MRI for tissues characteristics analysis
F
Thank you both @Khaled Sleik and @Ahmed Torshani for your great input. I discussed the case with a cardiothoracic surgeon and an imaging cardiology colleagues. The differential diagnosis was largely in favor of tumor. They leaned towards "fibroelastoma" given the fact it is very close to the valve, and the very smooth rounded edges on both CT and TEE, although fibroelastoma is typically on the left side. Our imaging expert thought even after MRI we may not be very conclusive.
We decided to start on Xarelto empirically (given high DD) and will repeat imaging (CT) in 3 months. After this discussion, I will discuss the PET option with my imaging colleague.
Will keep this post updated ISA.
Can we see real live video of the TEE
F
I attached a quick video with images above. As you can see pulmonary artery is very anterior and TEE doesn't always show perfect details.
I don't see the video
The good news is that the lesion is on the right side of the heart. Lungs could handle this but brain/other organs not.
I would have done the same with short term anticoagulation and repeat TEE in 8 weeks.
Although, unlikely to resolve with anticoagulation. I agree it is mostly likely fibroelastoma. Sarcoma usually invades the wall. Elevated d dimer could associated small thrombus on the top of the mass. Curious what repeat d dimer would be in 3 months
F
tnx. @Mansour Khaddr . Will update you with images later ISA.
I see the video now
it is likely myxoma
F
Unusual site for myxoma too.
I think it doesn’t matter if it was myxoma or fibroelastoma as long as it is not metastatic/malignant lesion which is unlikely.
I have seen cases of left atrial sarcoma, aortic valve fibroelastoma and mitral valve fibroelastoma.
In terms of metastatic lesions: I saw metastatic melanoma and lung cancer